Cure To OA Right Under Our Noses
Department of Biomedicine - University of Basel
Atharva Damle
Millions of people worldwide suffer from extreme pain and difficulty in walking, which is usually caused by wear of the knee cartilage. This degenerative disorder is termed Osteoarthritis (OA). Although it affects other joints like the hands and hips, knee OA contributes to the majority of cases. The symptoms of OA are apparent in the form of pain and inflammation in the knee but the changes in the body leading to OA are significantly complex. Overcoming this complexity has posed an untreatable challenge to biomedical researchers and clinicians for decades. So far, the biological and pharmacological options are limited and have only been able to postpone cartilage degradation, but not prevent it. Hence, patients suffering from end-stage OA, where all non-surgical treatment options have failed, are prescribed for partial or total knee replacement.
The Good, the Bad and the Ugly
Imagine two lubricated mechanical gears sliding against each other. This movement is analogous to that of two bones of the knee joint covered with a lubricating cartilage surface. Applying the analogy of sliding gears to treating OA, a knee devoid of cartilage is replaced with metal components. Between these two metal components, a plastic spacer acts as a cartilage replacement. After a surgical intervention like this, it might take months to fully recover. Most patients undergoing knee replacement enjoy a pain-free life. However, there might be some problems associated with using implants for the treatment of OA.
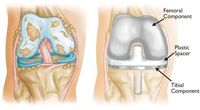
Figure 1: (Left) Severe osteoarthritis. (Right) Knee after a Replacement Surgery1
Implants used for knee replacement surgeries typically have a 15–20-year lifespan. Due to increased life expectancy and a sedentary lifestyle, the next generation may have to undergo multiple knee replacement surgeries. With the growing population of the world, this can put a significant socioeconomic burden. Additionally, knee replacement surgeries carry the risk of implant-associated infections and loosening, which although rare, can be challenging to manage and often require revision surgeries. To address these problems, researchers have been exploring other alternatives and are trying to move away from implants.
A Regenerative Renaissance
Along with the problems accompanying replacement surgeries, scientists have been grappling with the treatment's philosophy of simply replacing the degenerated cartilage with a foreign object instead of regenerating it. An alternative suggests using the regeneration power of your own cells (autologous) to reconstruct cartilage. Think of a lizard growing its tail back. This may sound easy, but cartilage cells of the joint or articular chondrocytes, have a poor regenerative capacity, especially where age is a limiting factor. Thus, therapies to repair knee defects based on implanting healthy autologous cartilage into the damaged area resulted in limited success.
To overcome these problems, scientists are working on utilizing the regeneration potential of Mesenchymal Stem Cells (MSCs). Simplistically speaking, MSCs are special cells that can transform into different cell types, including chondrocytes when induced by specific signals. Moreover, they help maintain and repair our connective tissues with their unparalleled regeneration capacity. Moreover, articular cartilage is developed from MSCs during human development. Various approaches have been developed to exploit their self-renewal and regenerative power for cartilage repair. These include an injection of MSCs in the knee defect, which then gets matured into cartilage by the signals provided by the surrounding environment. MSCs can be isolated from the patient and induced to form a cartilage graft by providing certain extrinsic signals in the laboratory. The generated graft can then be implanted in the knee defect of the patient. Such reconstructed cartilage from cells is termed tissue-engineered cartilage. Nevertheless, there is significant variation in the quality and reparative ability of cartilage constructed from different sources of MSCs. Although MSCs are potentially safe, it is a topic of investigation to standardize the cell source and the dosage of cells to establish a clinical procedure for cartilage regeneration2.
Pinocchio’s Remedy
Nasal chondrocytes (NCs) might be the most promising candidate among autologous regenerative cell sources. NCs have a higher self-renewal capacity than articular chondrocytes. Moreover, harvesting nasal cartilage is much less invasive than harvesting MSCs, with minimum damage to the nasal septum providing a standardized and reproducible source for regenerative cell therapy.

